16 Codes Became 46 in 2026. Physicians Must Document Differently, Starting Now.
The most significant overhaul to lower extremity revascularization coding in over a decade is already in effect.
As of January 1, 2026, CMS updated the existing lower extremity revascularization code set with 46 new codes that require substantially more documentation precision from physicians. Programs that do not adapt could undercode complex cases, lose revenue, and risk submitting claims that cannot be supported by the documentation.
Here's what's changing and exactly what physicians need to document in every case.
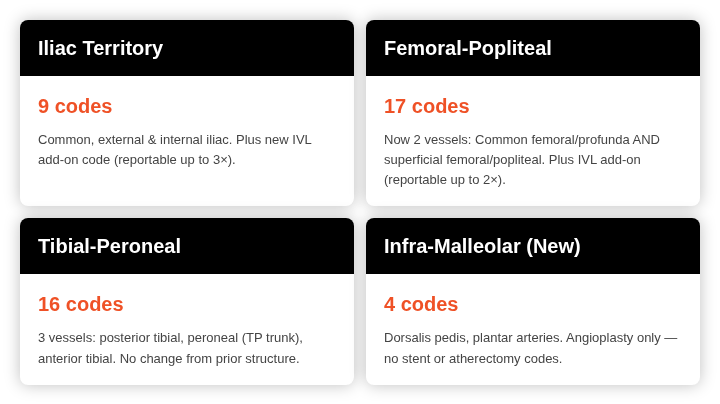
The New Territory Structure
Two structural changes shape the 2026 lower extremity revascularization code set. The femoral-popliteal territory has been split into two separate vessels: common femoral/profunda and superficial femoral/popliteal, requiring physicians to document each vessel independently. And for the first time, procedures performed below the ankle have a dedicated territory: infra-malleolar, covering the dorsalis pedis and plantar arteries. The result is four distinct territories, each with its own code family. Vessel-level documentation is no longer optional; it is what determines the code.
The 3 Documentation Must-Haves For Lower Extremity Cases
1. Exact anatomic location of lesion
The specific vessel name matters. Common femoral and superficial femoral are now different code territories. An intervention extending from the popliteal into the TP trunk codes to the TP trunk, not popliteal. Vague references like 'the femoral artery' are no longer sufficient. Be precise.
2. Numeric percent stenosis
Lesions that are 50–99% stenosed are classified as "straightforward" and generate lower RVUs, while 100% occluded lesions are classified as "complex" and generate substantially higher RVUs. The term "occluded" should only be used to describe a 100% lesion, but documenting a numeric stenosis is always the safest approach to avoid ambiguity.
3. Intervention type and location
The code hierarchy: stent with atherectomy > atherectomy > stent > angioplasty. If intravascular lithotripsy was used, it must be explicitly documented as a separate add-on. Each distinct territory can generate one initial interventional code, plus add-ons.
.png)
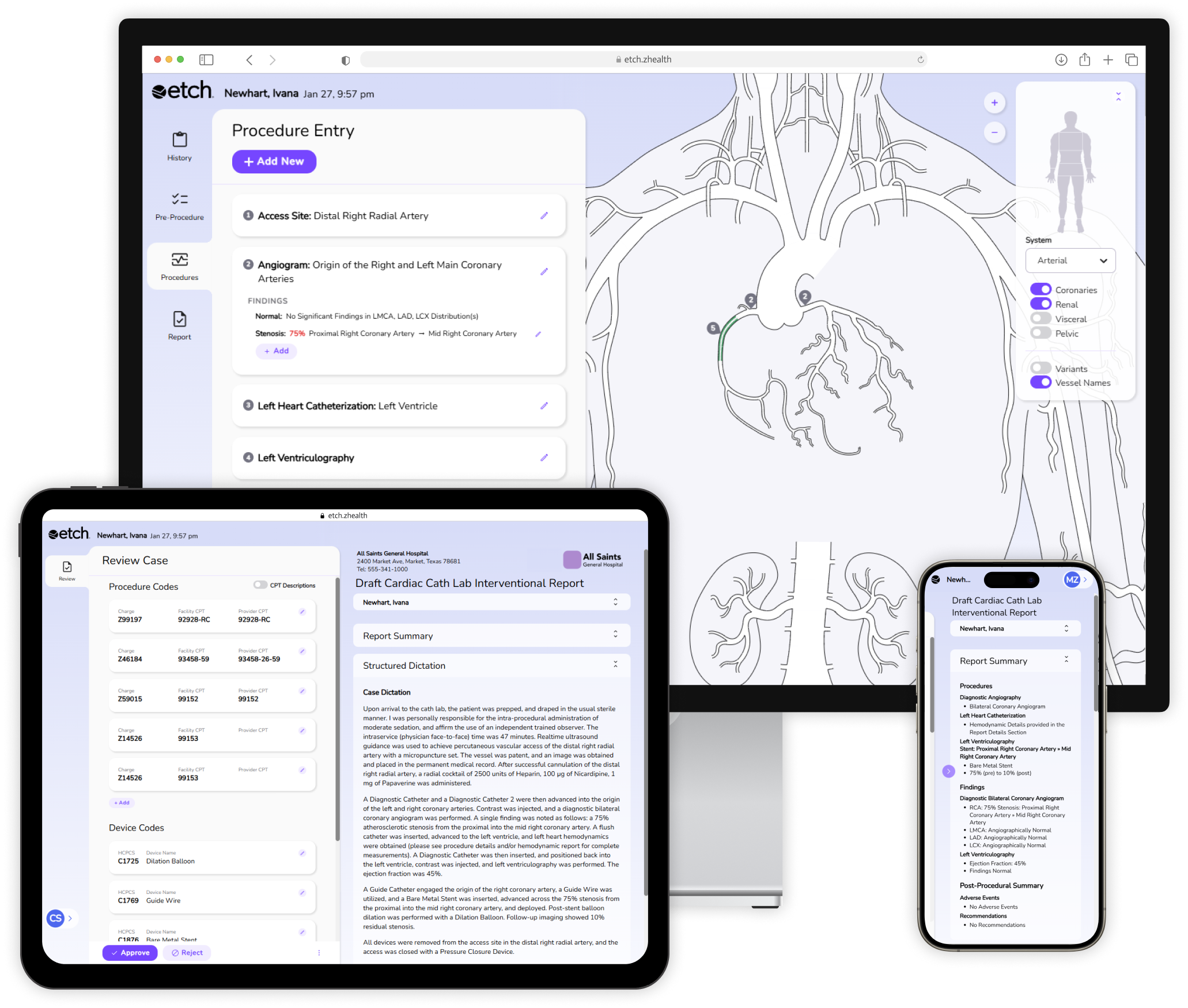
The Etch Effect
Etch is purpose-built around the 2026 CPT coding updates for lower extremity revascularization. As physicians document, Etch guides them through the specific clinical details that determine code assignment, including stenosis documentation, exact vessel location and territory, and interventional procedures. Once documentation is complete, Etch automatically applies the correct codes. As coding requirements change, Etch updates in the background, protecting your program from compliance risk and revenue leakage without disrupting your workflow.